
April Tip of the Month - Vector Change
At any point a patient has had three (3) consecutive defibrillations, paramedics shall consider a vector change prior to the next defibrillation. If the first set of pads applied are placed in the anterior/lateral position, the second set of pads shall be placed in the anterior/posterior position. Note: the first set of pads may remain in place but need to be disconnected from the monitor. Once the second set of pads are applied in the anterior/posterior position, ensure that you connect them to the defibrillator.
If subsequent defibrillations are performed, and the patient remains in refractory VF or pulseless VT, paramedics shall then initiate extrication and transport early once an egress plan has been established.
For Primary Paramedics: After 3 consecutive shocks while using vector change defibrillation (VCD)
For Advanced Care Paramedics: After 3 consecutive shocks while using vector change defibrillation (VCD) AND administration of 3 rounds of epinephrine (or after 3rd consecutive defibrillation if no IV/IO/CVAD/ETT access).
Conversely, if the patient is converted to a non-shockable rhythm (PEA/Asystole), paramedics shall remain on scene and continue resuscitation (up to 20 mins) as per the cardiac arrest medical directive.
Careful pad placement allows for the most direct and unobstructed path of transthoracic current (TTC). Improper pad placement and the presence of a variety of substances can create resistance to current flow, also called transthoracic impedance (TTI). Some examples that may interfere with the delivered current and create impedance, or resistance, may include jewelry, hair, moisture and breast tissue.
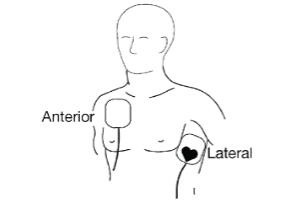
When pads are placed anterior-laterally, or standard placement, one pad is placed on the patient’s upper right torso above the right nipple (just below the clavicle), and the other pad should be placed lateral to the patient's left nipple, with the center of the pad on the midaxillary line, where possible. See the following image below for detail.
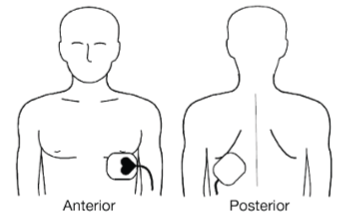
Alternatively, for the anterior-posterior position, or front-back position, place the front pad over the cardiac apex between the midline of the chest and nipple on a male victim or under the breast on a female. The posterior pad should be placed to the left of the spine just below the scapula at the heart level. See image below.
The following are examples of appropriate documentation when applying new defibrillation pads:
