
February Tip of The Month - 12 lead interpretation Week 3 RESULTS
This week we will review and provide “answers “from last week's cases. The quotations are important. There is no expectation that you would be out in the field definitively determining what each of these ECGs is about. You will always be using clinical judgment based on context, the nature and severity of the patient's condition, and underlying comorbidities. As we always say with ECGs… one begets another! Always consider doing repeat ECGs to look for the evolution of change. This can provide the most important clue.
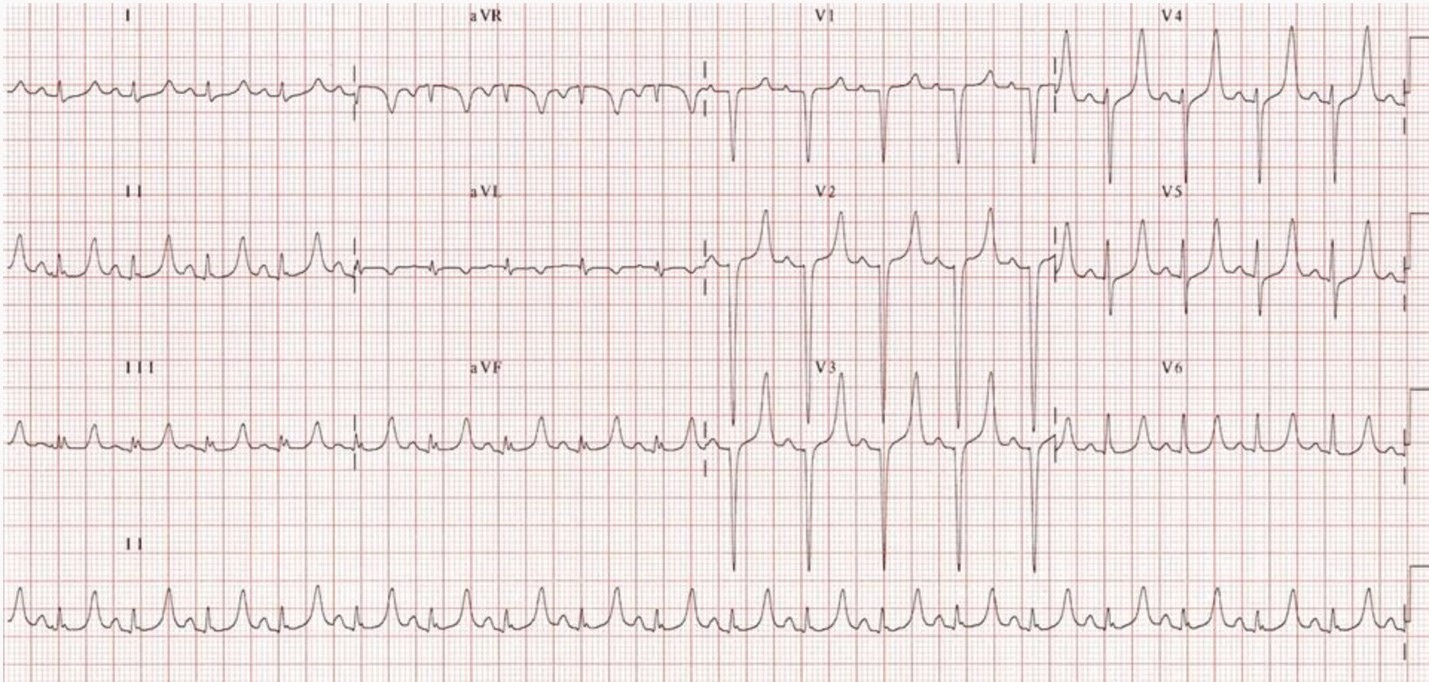
ECG 1 - Left Ventriuclar Hypertrophy (LVH)
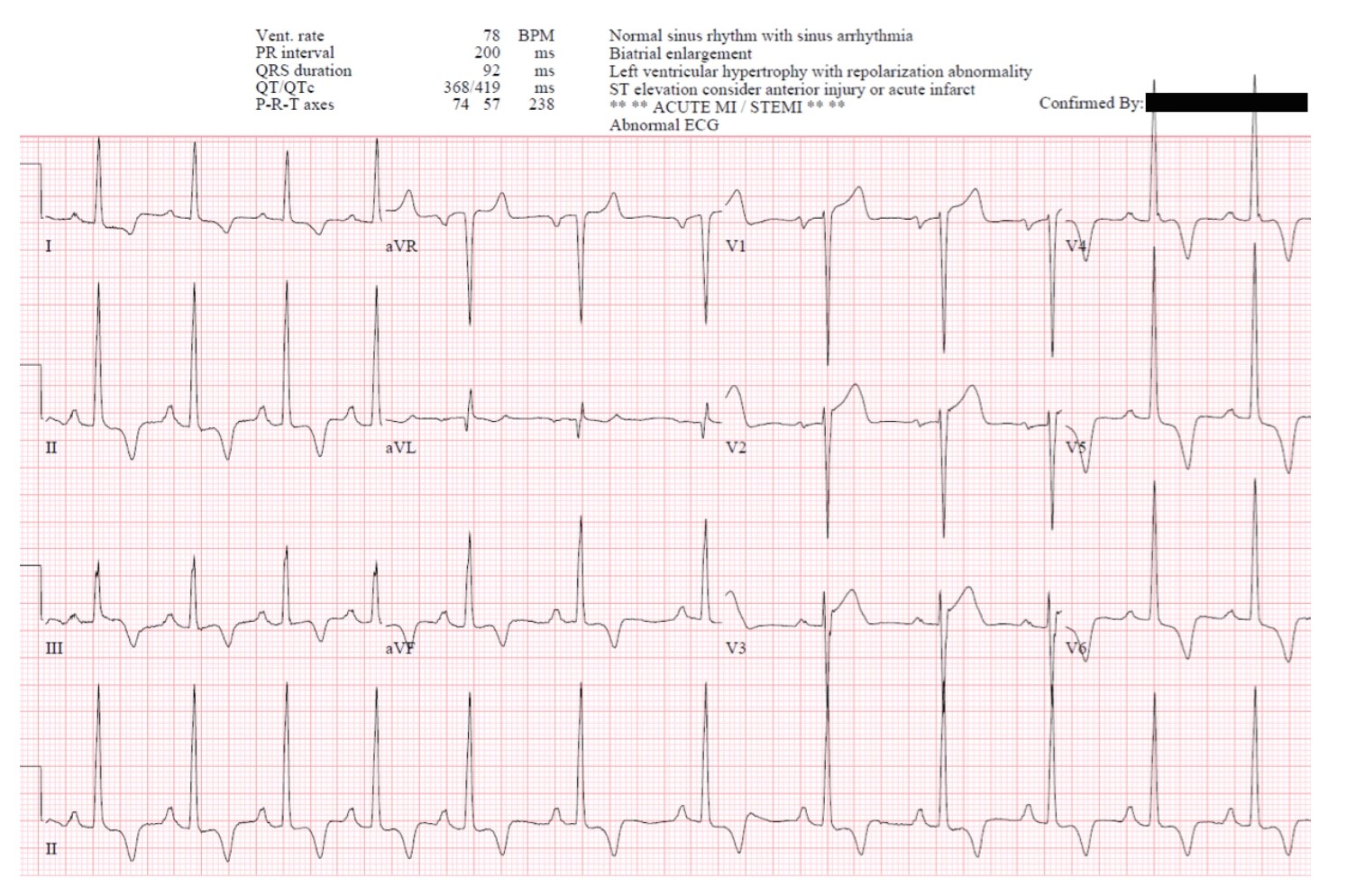
R wave in lead I + S wave in lead III > 25 mm
R wave in aVL > 11 mm
ST segment depression and T wave inversion in the left-sided leads: AKA the left ventricular ‘strain’ pattern
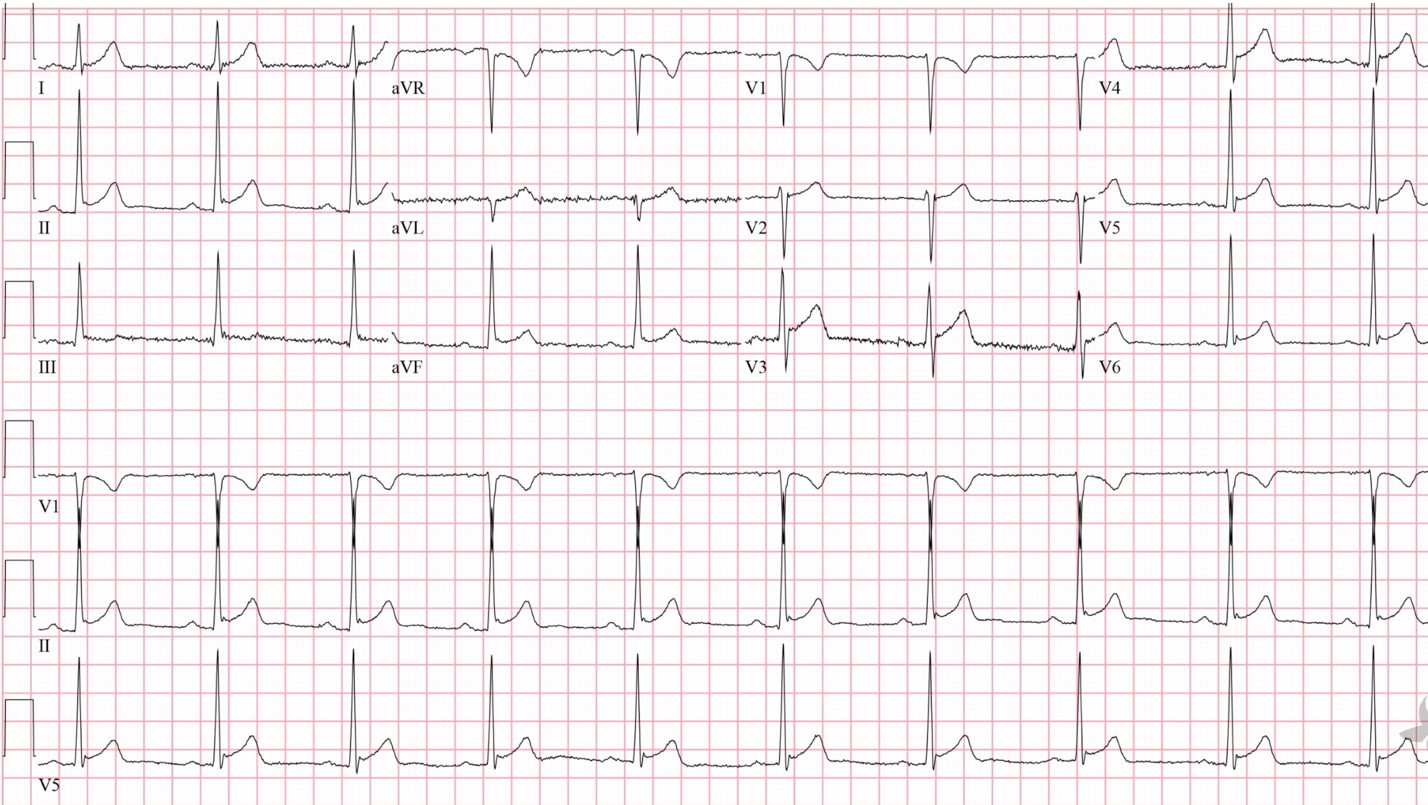
ECG 2 - Hyperacute T waves (HATW)
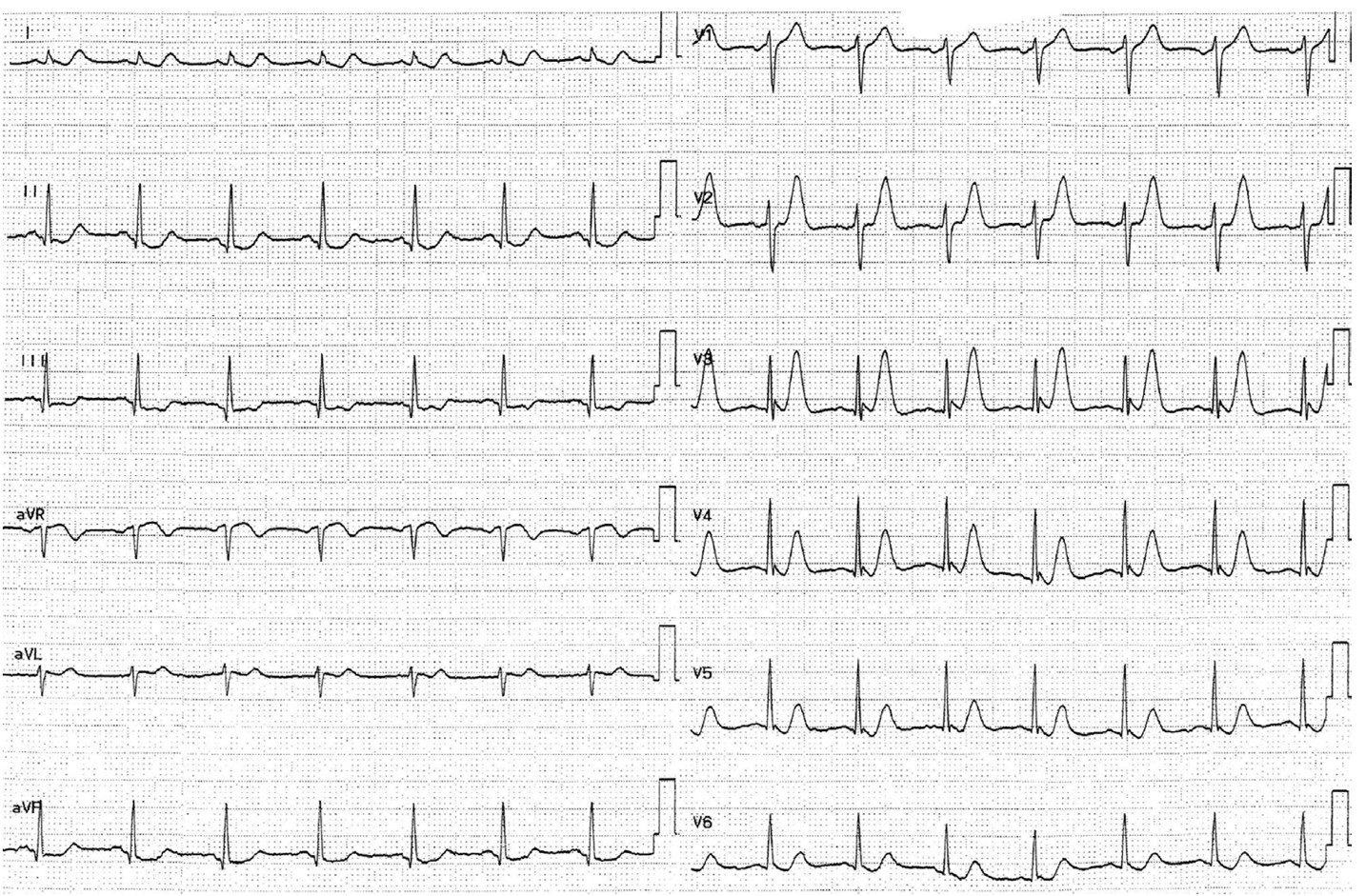
There is no accepted definition for HATW. They are generally broad-based, and symmetric. The ratio of the area under the T wave compared to the QRS amplitude i.e., PROPORTIONALITY is key. These can be the earliest indication of a STEMI. Look for a straight initial slope instead of a concave, “smiling” contour.
If the T wave is larger than the entire QRS think about HATW.
Remember, never rely on a single ECG.
In example 2, note the size of the T waves across the precordium (the portion of the body over the heart and lower chest), particularly in V3. There is also reciprocal inferior STD. This is very concerning ECG that turned out to be an LAD occlusion
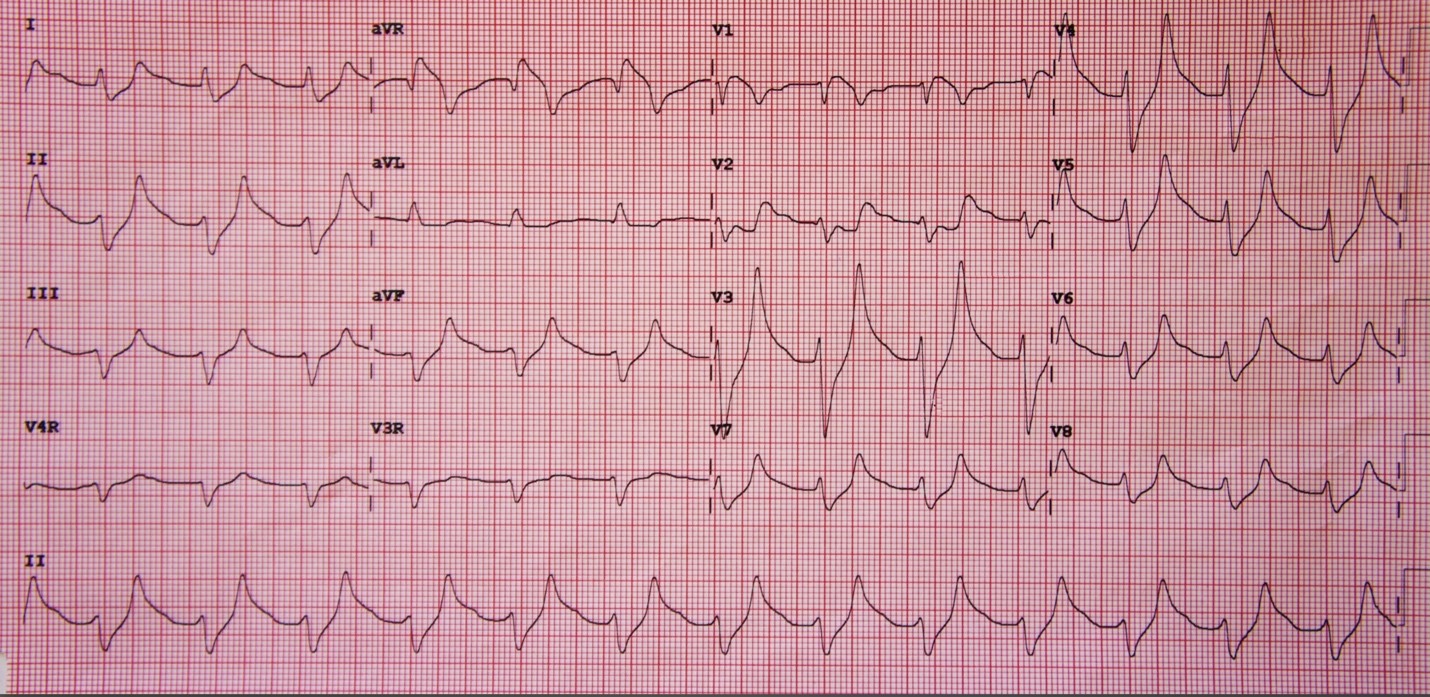
ECG 3 - Hyperacute T waves (HATW)
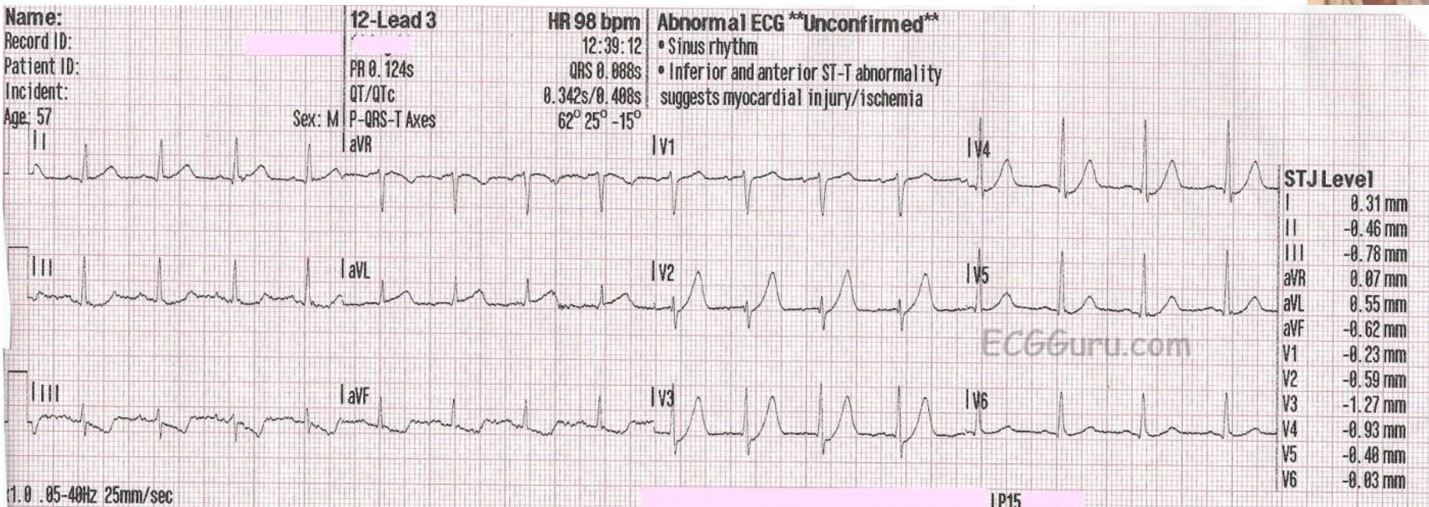
Here again, we see very large T waves across the precordium. There is a bit of STD before the takeoff of the T wave in V2 and V3, known as deWinter T waves and indicative of LAD occlusion. Once again there is reciprocal STD in the inferior leads.
ECG 4 - Left Bundle Branch Block (LBBB)
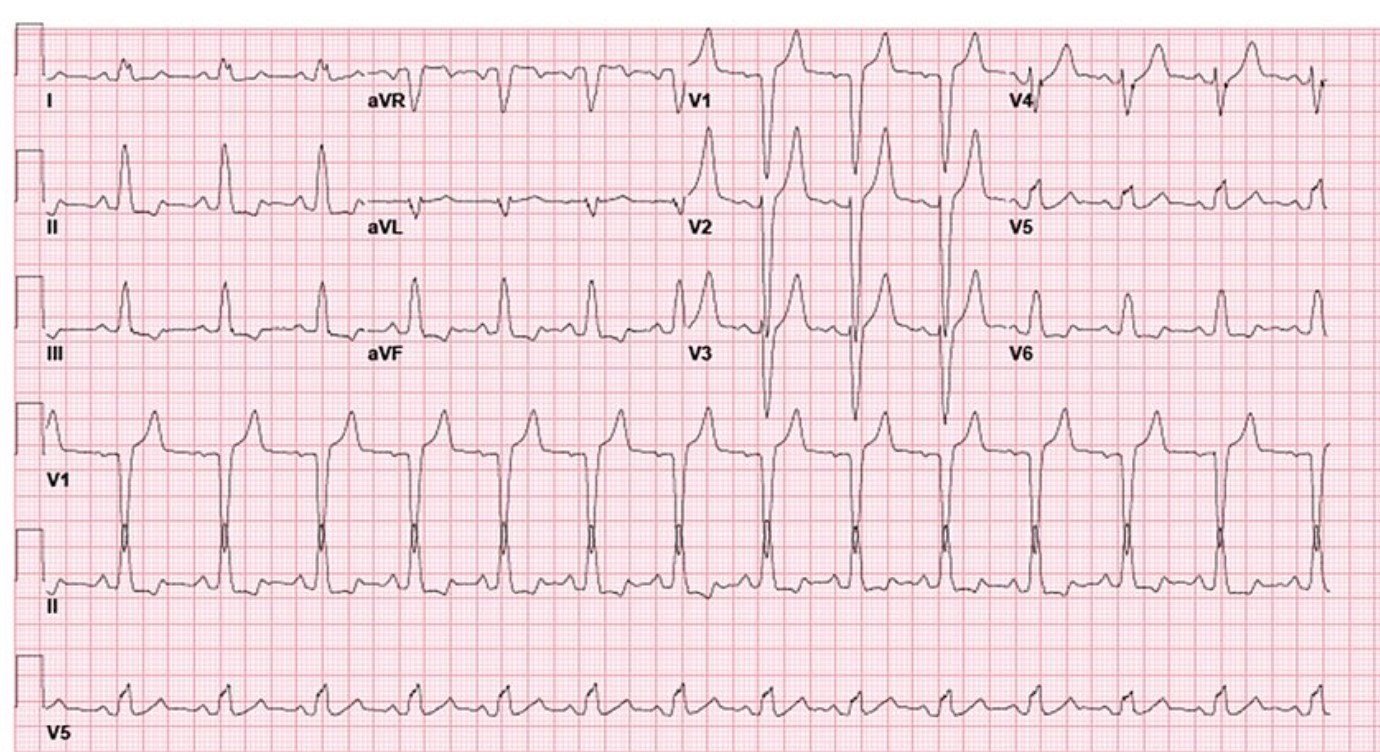
Here we have typical LBBB findings…
- QRS duration ≥ 120ms
- Dominant S wave in V1
- Broad monophasic R wave in lateral leads (I, aVL, V5-6)
- Absence of Q waves in lateral leads
There are no Sgarbossa criteria to suggest ischemia.
ECG 5 - Hyperkalemia
Now those are “peaked” T waves!! No reciprocal changes. Again, context might be definitive in your evaluation.
ECG 6 - Benign Early Repolarization - BER
BER diagnosis criteria are below, but always by exclusion with serial ECGs and looking for reciprocal changes!
- Widespread concave ST elevation, most prominent in the mid-to-left precordial leads (V2-5)
- Notching or slurring at the J point ( lead II)
- Prominent, slightly asymmetrical T waves that are concordant with the QRS complex
- No reciprocal ST depression to suggest Occlusion MI
ECG 7 - Hyperkalemia
This one is classic!! Wide QRS, loss of P waves, HUGE T waves…. but always put in context.
That is all for now…”see” you next week!