
February Tip of The Month - 12 lead interpretation Week 2 RESULTS
Week 2 ECG Challenge – Results & Analysis
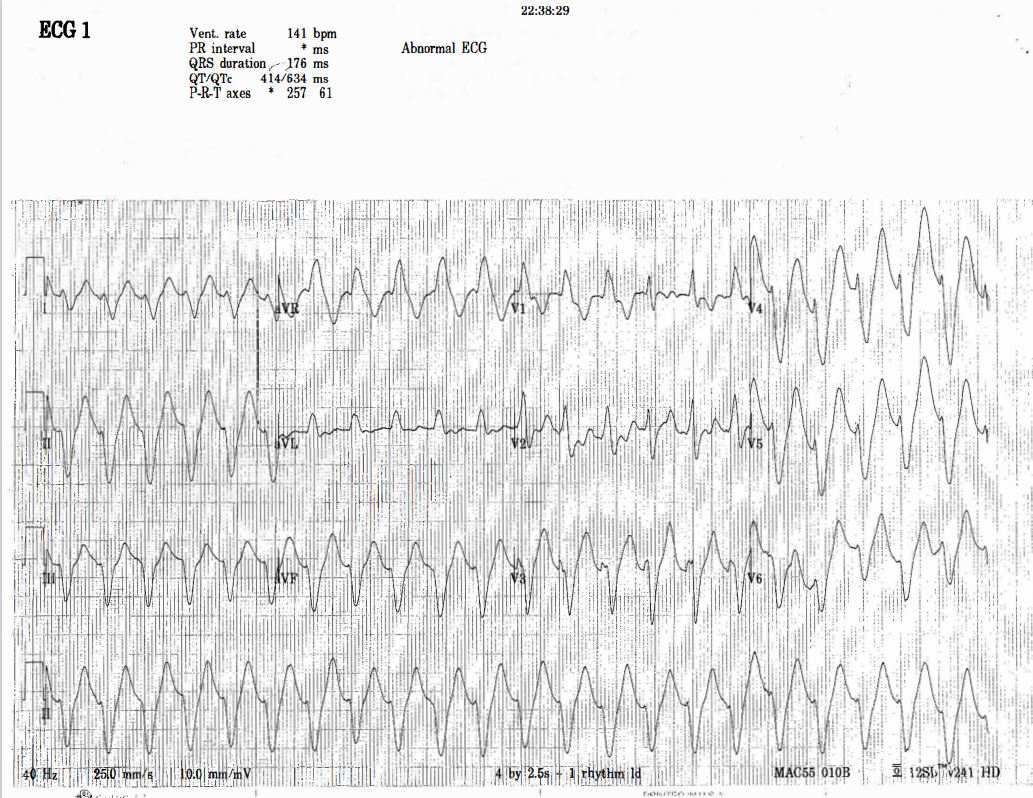
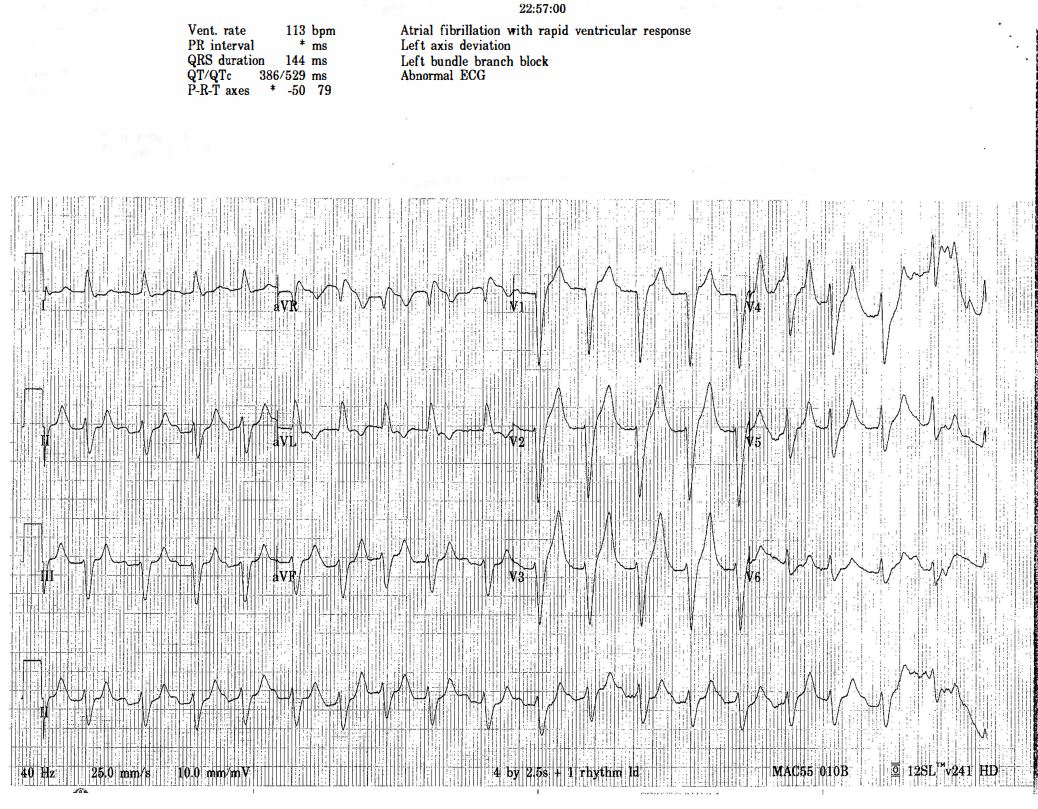
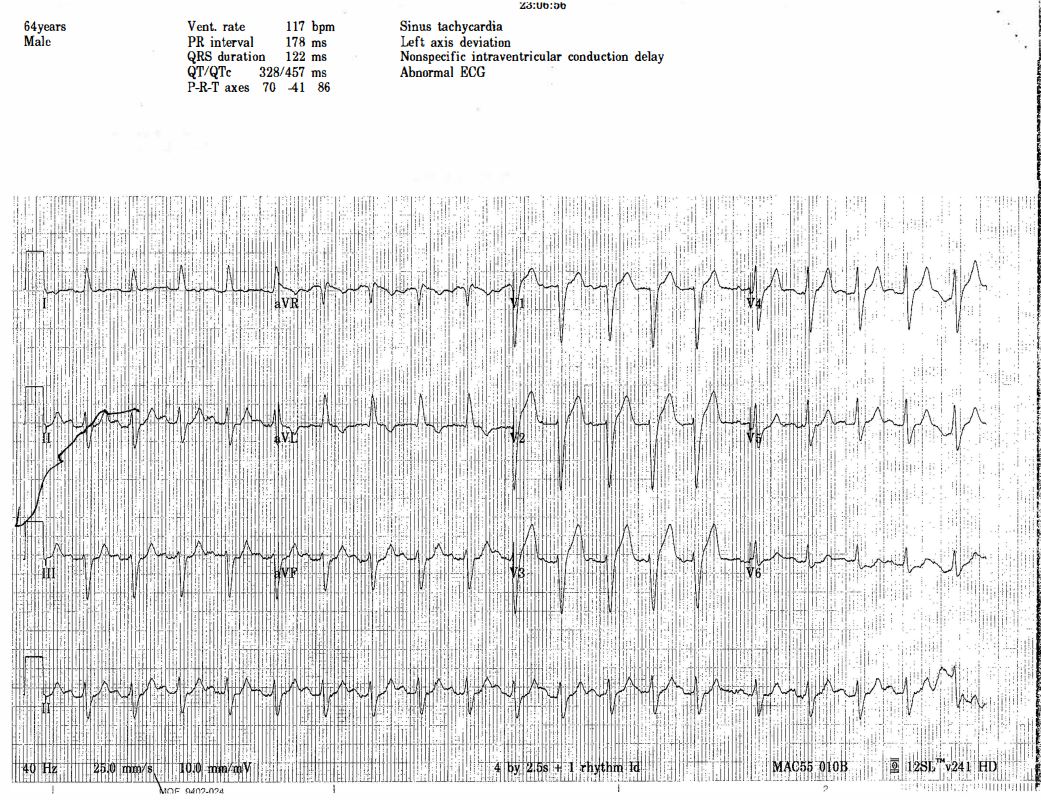
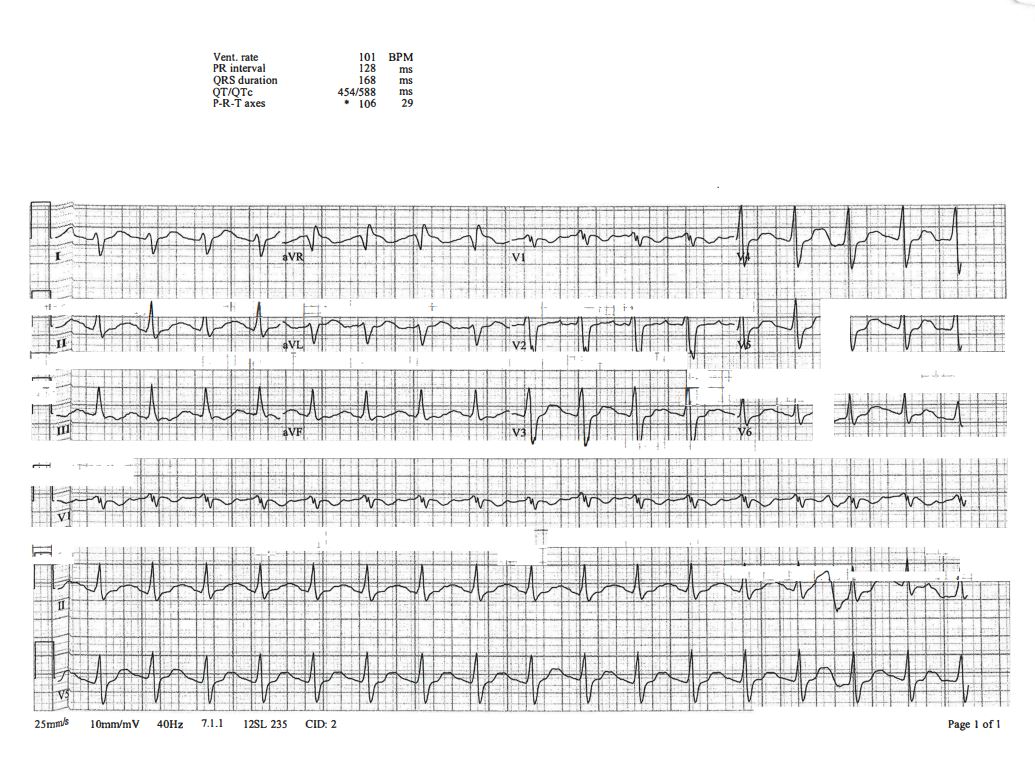
ECG 1 – Corresponds to Case C
- Key observation: Note the time of the first ECG (22:38) and how the ECG changes over the next 30 minutes.
- What happened? The ECG initially resembles ventricular tachycardia (VT) but rapidly narrows to sinus rhythm within 30 minutes.
- What treatment works this quickly? No "shifting" medication acts this fast—only calcium can cause such rapid stabilization. This patient received four amps of calcium gluconate.
- Clinical presentation: This patient exhibited Kussmaul’s breathing, a deep and labored respiratory pattern associated with metabolic acidosis.
- Hospital findings:
- Potassium (K⁺): 7.6
- pH: 6.91
- HCO₃: <5
- ECG 1: 1 of 3
- ECG 1: 2 of 3
- ECG 1: 3 of 3
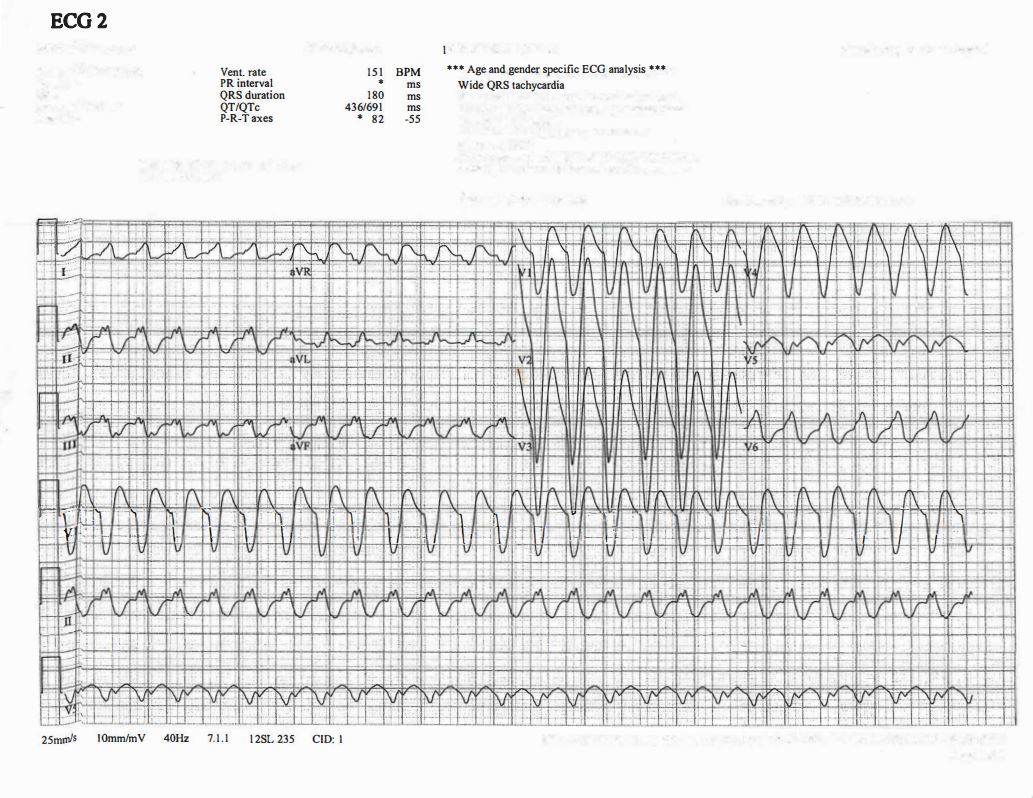
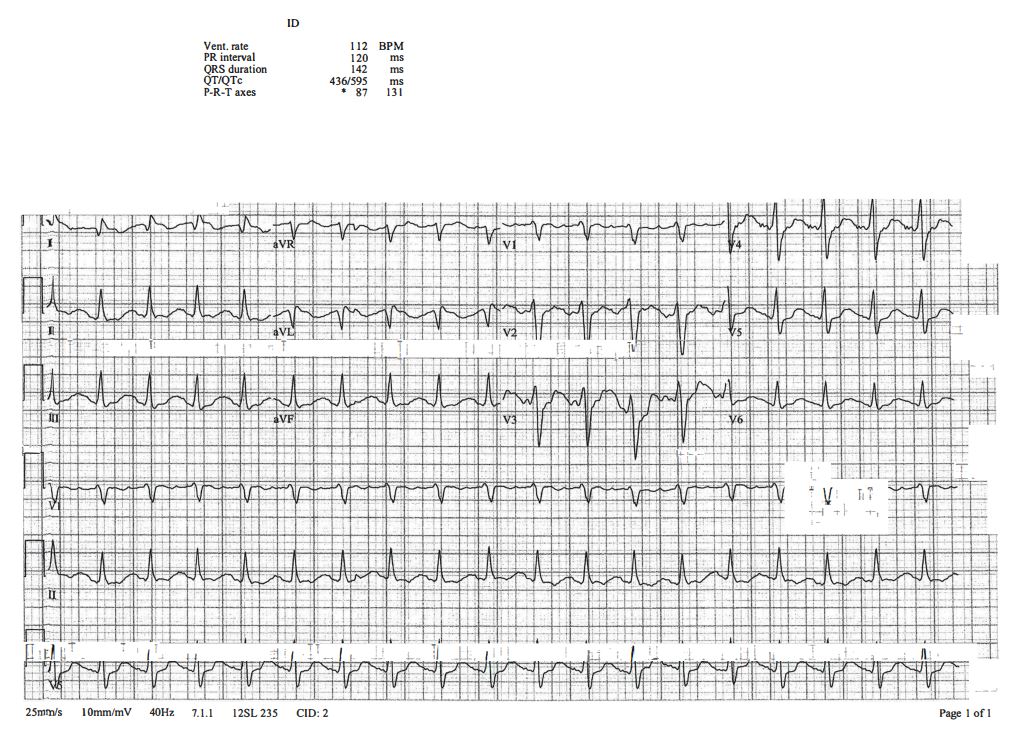
ECG 2 – Corresponds to Case A
(From the LITFL library)
- This ECG displays features of sodium-channel blockade, commonly seen in tricyclic antidepressant (TCA) overdose and other toxicologic causes.
- Key ECG findings of sodium-channel blockade:
- Intraventricular conduction delay: QRS >100 ms in lead II
- Terminal R wave >3 mm in aVR or R/S ratio >0.7 in aVR
- QT prolongation
- Sinus tachycardia (often seen in TCA overdose due to muscarinic receptor blockade)
-
ECG 2 Features of Sodium-Channel Blockade (image)
- How wide is too wide?
- QRS >100 ms → Predictive of seizures
- QRS >160 ms → High likelihood of ventricular arrhythmia
- These patients will not benefit from cardioversion—they require antidotal therapy with hypertonic saline or sodium bicarbonate (NaHCO₃).
- Examples of medications causing sodium-channel blockade:
- Tricyclic antidepressants (TCA)
- Antihistamines
- Beta-blockers (e.g., propranolol)
- Local anesthetics
- Carbamazepine, oxcarbazepine
- Phenytoin (Dilantin), lamotrigine
- Cocaine
- Treatment considerations: In severe cases, Lipid Emulsion Therapy (LET) may be used as an adjunct
- How wide is too wide?
- ECG 2: 1 of 3
- ECG 2: 2 of 3
- ECG 3: 3 of 3
-
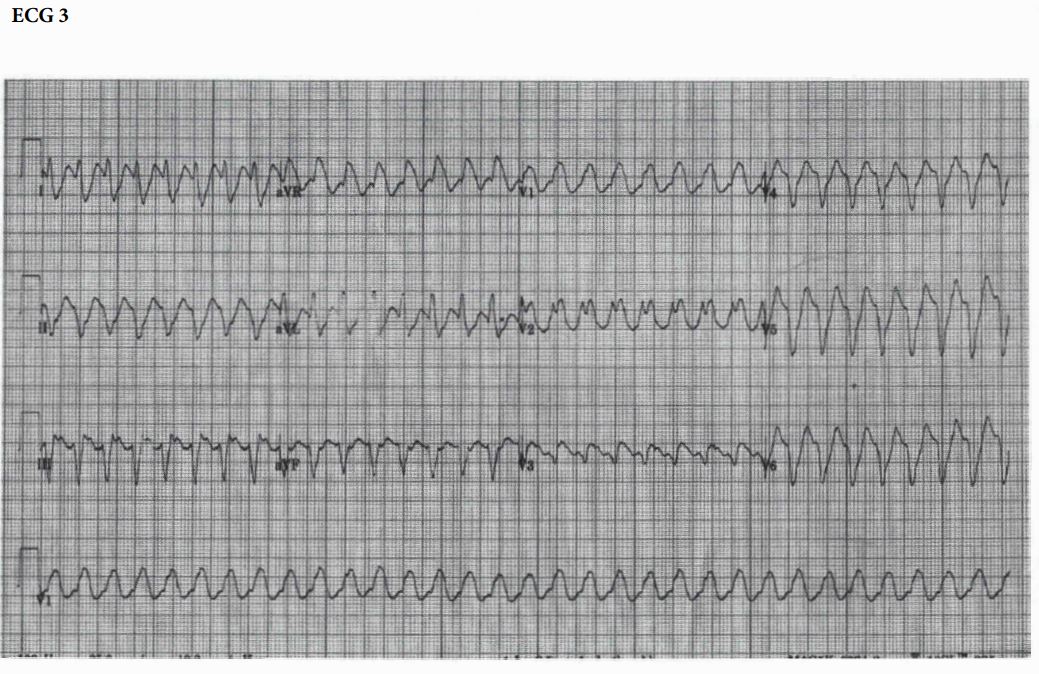
ECG 3 – Corresponds to Case B
- This ECG represents stable ventricular tachycardia (VT)—for now.
- Management considerations:
- The patient requires immediate cardiac monitoring and defibrillation pads in case of deterioration.
- Unstable VT → Immediate synchronized cardioversion.
- Stable VT → Antiarrhythmic therapy (e.g., Amiodarone).
- Likely cause: This is ventricular scar-mediated VT, often associated with prior myocardial infarction (MI) and ischemic heart disease.
- ECG 3 Image
Summary & Key Takeaways
When faced with a wide complex tachycardia (WCT), always consider:
- Ischemia
- Drugs & toxins (e.g., prolonged QT, polymorphic VT, sodium-channel blockade)
- Metabolic causes (e.g., hyperkalemia, acidosis)
At first glance, these three ECGs all resemble VT, highlighting the importance of:
✅ Taking a thorough patient history
✅ Contextualizing the scenario
✅ Recognizing metabolic and toxicologic ECG patterns
Each of these cases demonstrates the critical role of ECG interpretation in guiding patient management and ensuring appropriate treatment decisions.
Thank you for participating in this week's ECG Challenge! Stay tuned for next week’s case.