July Tip of the Month - Keys to Trauma Cardiac Arrest Management
Traumatic cardiac arrest (TCA) in the pre-hospital setting demands immediate, specialized management by paramedics. TCA can result from blunt trauma (e.g., motor vehicle collisions, falls) or penetrating trauma (e.g., stab wounds, gunshot wounds). Management starts with a rapid C-ABCDE assessment to identify life-threatening injuries. Prioritize interventions based on clinical relevance, addressing reversible causes like hypoxia, tension pneumothorax, and hypovolemia per ALS/BLS Patient Care Standards. Airway management, utilizing basic or advanced adjuncts, is crucial but should not delay transport.
Ensure adequate oxygenation and ventilation, addressing tension pneumothorax with needle decompression, if authorized. Bilateral needle thoracentesis should be considered for all traumatic arrests with chest trauma when indications are met. Control hemorrhage with direct pressure, tourniquets, or hemostatic agents, and establish vascular access for fluid therapy where applicable. In blunt TCA, apply a pelvic binder, when indicated, after addressing other reversible causes, or earlier if a pelvic fracture is suspected. Consider an intravenous fluid bolus if it does not delay transport, using large-bore IV or IO access for a 20 mL/kg bolus.
Continuous monitoring of cardiac rhythm, oxygen saturation, and end-tidal CO2 is essential. Consider delaying chest compressions until preload and obstructive causes are addressed. Rapid transport to a trauma center with surgical capabilities is critical for definitive care.
The termination of resuscitation criteria for traumatic cardiac arrest includes specific conditions.
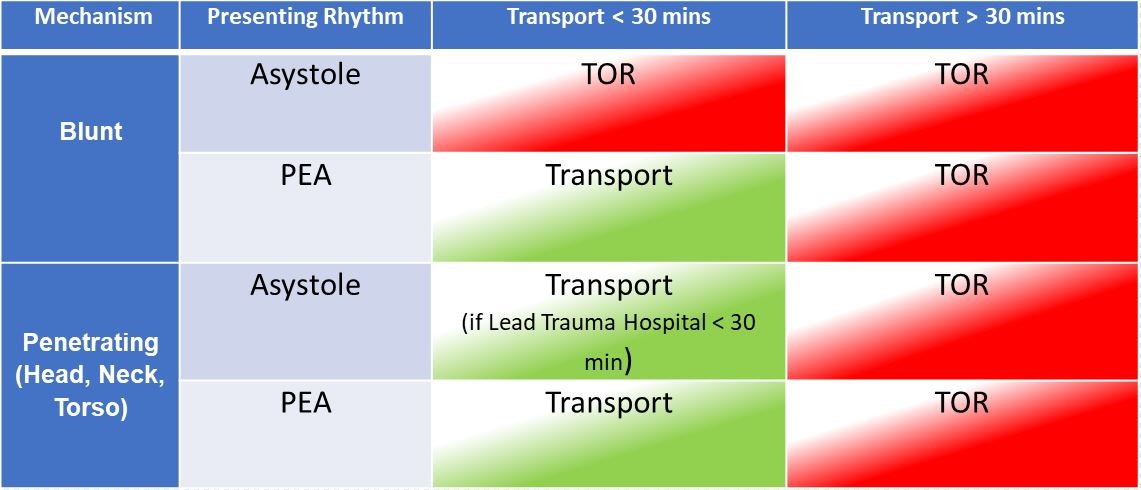
Patients aged 16 or older with no heart rate or breathing, and asystole are generally signs of poor viability and meet the threshold for TOR consideration. Additionally, if there are no detectable pulses, no defibrillation given, and no signs of life since extrication, or signs of life but the nearest hospital is over 30 minutes away, resuscitation efforts may cease following a BHP TOR order. The same applies if the patient presents with pulseless electrical activity (PEA), however, the closest hospital is more than 30 minutes away.
The TOR criteria is designed to help guide paramedics on when to call for TOR consideration, , ensuring resources are used effectively and care aligns with realistic outcomes.
Paramedics are encouraged to utilize the table below to assist in determining if a patient meets TOR criteria.