February Tip of The Month - 12 lead interpretation Week 1 RESULTS
Answers:
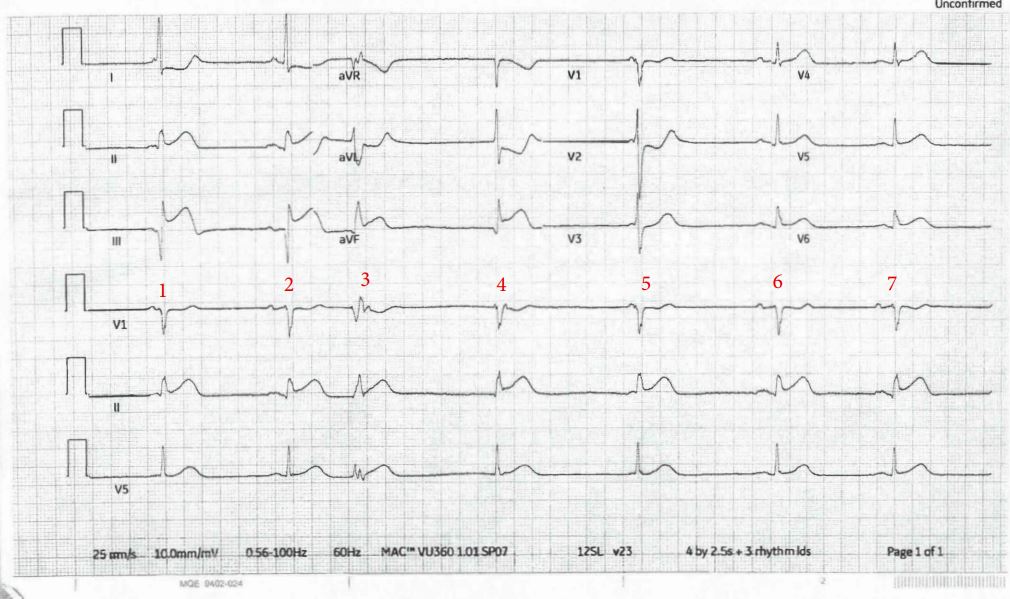
- The rhythm strip at the bottom using V1 gives us our best chance for accurate interpretation (see ECG 1 below). V1 is always a good bet when you are looking for P waves. Beats 2, 6, and 7 show consistent PR intervals and QRS complexes; this is the underlying sinus rhythm. Beat 3 is a PVC followed by a pause and a junctional escape beat (4). Beats 1 and 5 represent junctional beats with retrograde P waves. These P waves are too close to the QRS to be conducted.
- There is ST elevation in leads 2, 3 and aVF. There are tall R waves in V2 and V3 with ST depression. This is an inferior-posterior myocardial infarction (MI).
- There are reciprocal changes in leads I and aVL.
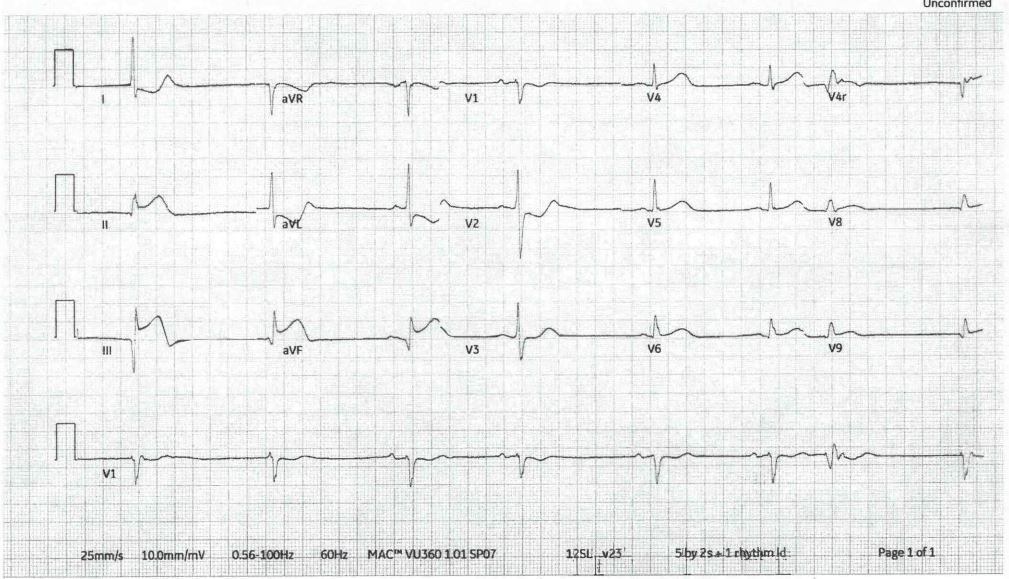
- The additional test is a 15-lead ECG (see ECG 2 below). Here, we see STE in V8 and V9, consistent with posterior wall involvement. Note that it is not necessary for the 15 lead to be positive to confirm posterior wall involvement. The first 12 lead has enough information. Also, note that V4r shows some subtle ST elevation, indicating right ventricular wall involvement. This represents a serious MI with significant morbidity/mortality.
Additional information:
When documenting on your ACR, the appropriate interpretation of the 12 lead is:
- Inferior-posterior STEMI with a sinus rhythm at approximately 40 bpm. STE in lead II, III, aVF, reciprocal changes in I and aVL and ST depression in V2 and V3. PVC’s and junctional escape beats are also present.
ECG 1
- ECG 2 - 15 Lead