
Tip of the Month - April 2026 - Glasgow Coma Scale
"Can you open your eyes for me?"
If a patient opens their eyes when you speak to them, are they automatically a GCS 14?
Not necessarily. Accurate scoring depends on how and why the response occurs
Why This Matters
GCS miscalculations remain common in the field - particularly in Eye Opening and Motor Response scoring.
These errors can impact:
- Clinical decision-making
- Transport priorities
- Accuracy of hospital handover
Key Principles for Accurate Scoring
- Document the best observed response
- Score based on the highest level of function demonstrated
- Identify and communicate trends
- Serial GCS assessment are more valuable than a single score
- Differentiate inability vs. non compliance
- Is the patient unable to respond, or choosing not to?
- Baseline matters
- A patient who is baseline- oriented is a GCS 15, even with pre-existing cognitive impairment
The Golden Rule
A decreasing GCS is an early and critical indicator of patient deterioration.
Factors That Can Interfere with GCS Assessment
- Pre-Existing Conditions
- Language barriers
- Cognitive impairment or developmental delay
- Hearing or speech impairment
- Current Interventions
- Airway management (e.g., intubation, tracheostomy)
- Medications (e.g., sedation, analgesia)
- Acute Illness or Injury
- Facial, orbital, or cranial trauma
- Stroke symptoms (e.g., dysphasia, hemiplegia)
- Spinal cord injury
- Hypoxia
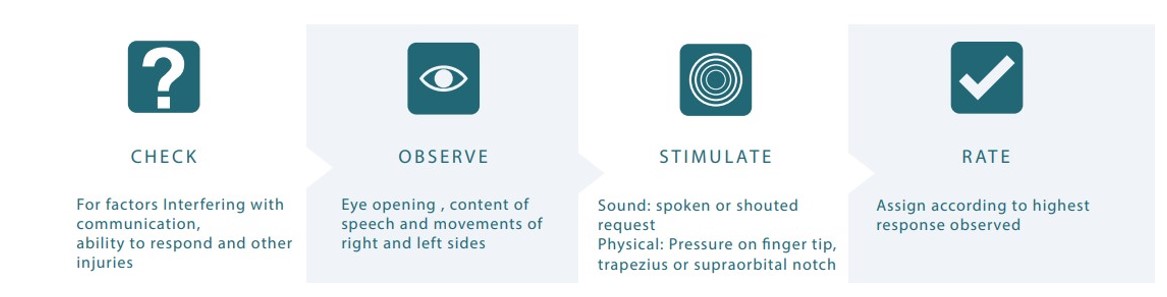
Approach to GCS Assessment 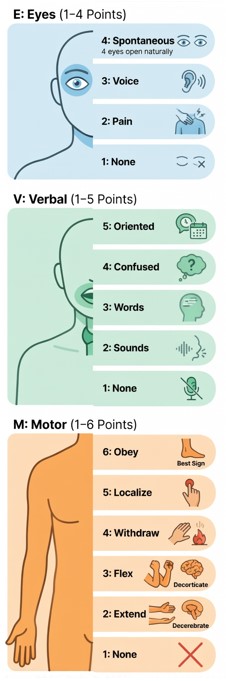
CHECK
Identify factors that may interfere with accuracy
OBSERVE
Look for spontaneous eye opening, speech, and movement
STIMULATE
Progress from verbal → tactile → painful stimuli (only as required)
RATE
Assign GCS based on the best observed response
Additional Resource
For further detail, refer to: Glasgow Coma Scale Foundation
glasgowcomascale.org