
June 2026 - Tip of the Month - Stroke Care Excellence
Mastering the Clock and the Card: Optimizing Field Stroke Assessments & Bypass Protocols
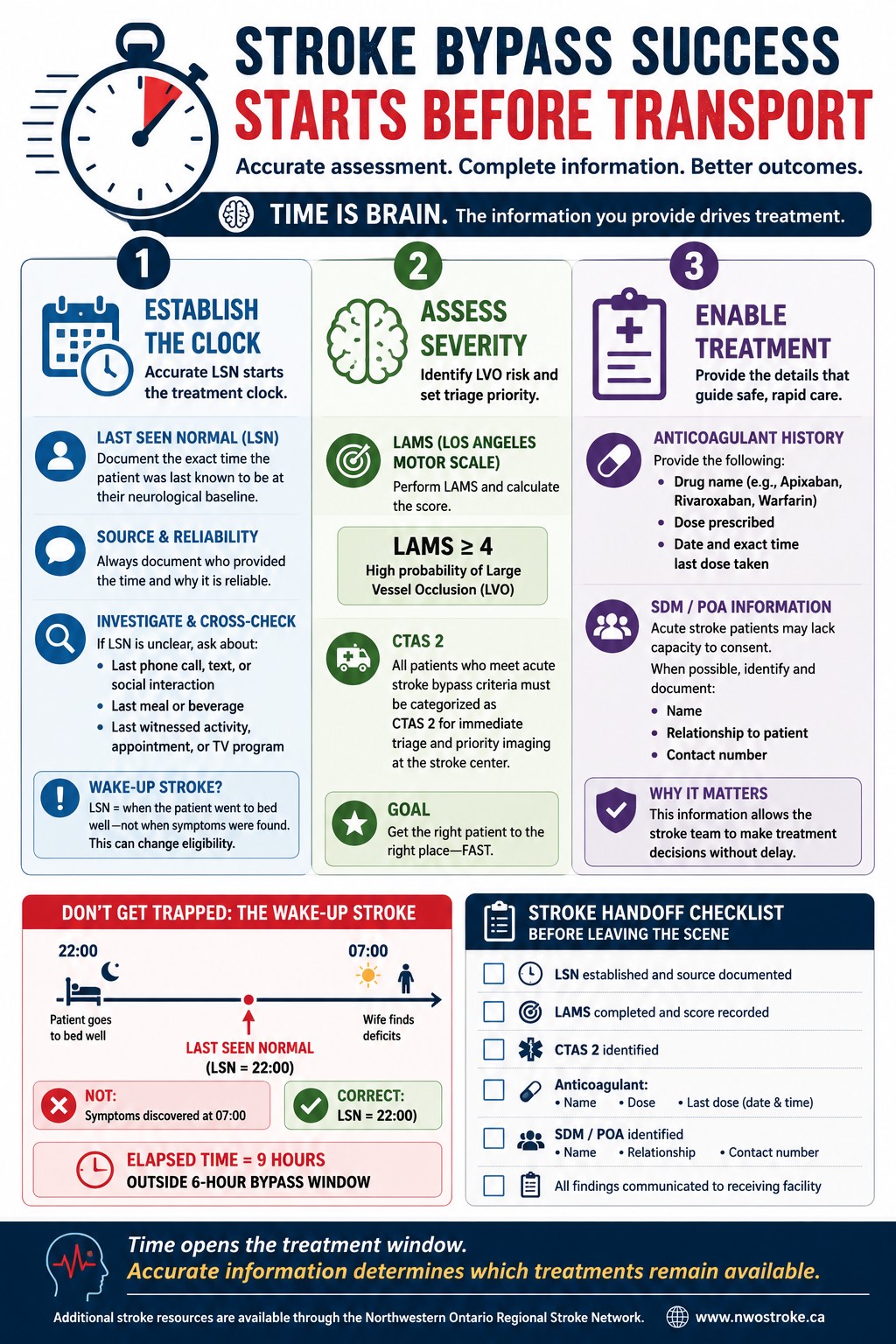
When an acute ischemic stroke occurs, millions of neurons die every minute, making rapid reperfusion therapy the highest priority. The Paramedic Prompt Card for Acute Stroke Bypass Protocol (see image below) acts as the guideline for this life-altering care, assisting paramedics to determine when to bypass local hospitals in favor of designated Regional Stroke Centers. However, the success of this hinges entirely on the quality of field assessment by paramedics. Accurate Identification of the Last Seen Normal (LSN) window, swift calculation of large vessel occlusion (LVO), and medical history are what allow the emergency department stroke teams to immediately assess and determine the appropriate treatment including the administration of thrombolytic medication like Tenecteplase (TNK) or other potential treatment pathways.
By the end of this tip, paramedics will be able to accurately calculate and document a patient’s LSN time, correctly apply the LAMS score for LVO screening, and gather the critical anticoagulant data required to optimize the acute stroke bypass.
You respond code Red to a 74-year-old male who is altered and nonverbal. His wife states, “He was fine when he went to bed. When I woke up at 07:00, I found him in bed; now he cannot speak or move his right side.” If you map the onset to 07:00, your 07:30 arrival makes him a candidate for the 6-hour bypass protocol. But when you ask what time he went to bed the night before, the wife replies, "22:00." Does this patient still qualify for the stroke bypass?
- The Last Seen Normal (LSN) Window & the “Wake up” Conundrum
The 6-hour timeline for the Ontario Acute Stroke Bypass Protocol is based strictly on the LSN time, which is the last moment the patient was confirmed to be at their neurological baseline - not when the symptoms were discovered.
- The Wake-Up Conundrum: As seen in our scenario, if a patient wakes up with symptoms, their LSN is the time they went to bed well (22:00), placing them at 9 hours and well outside the 6-hour bypass window.
- Investigation/History Gathering: If the LSN is ambiguous, dig deeper. Ask the family about the last phone call the patient made, their last text message, their last meal, or the last time they got up to use the washroom.
- Documentation: Never just chart a time. Always include the source to validate its reliability for the ED physician.
- Incomplete: Onset 07:00.
- Complete: LSN 10:00 per wife, who confirmed the patient was speaking clearly and walking normally. Symptoms found by wife at 07:00.
- Secondary Screening: LAMS & LVO Assessment
Your inclusion criteria do not stop at the timing of LSN. Paramedics must perform a secondary screen for Large Vessel Occlusions (LVO) using the Los Angeles Motor Scale (LAMS).
- If the calculated LAMS score is greater than or equal to 4, the patient has a high probability of a major arterial blockage requiring specialized intervention.
- Any patient meeting the acute stroke bypass criteria must be explicitly categorized as a CTAS 2 to ensure immediate triage and priority imaging upon arrival at the stroke center/ED.
- The Blood Thinner Factor and Consent Gathering
Obtaining anticoagulant history is just as time critical as getting the patient to the CT scanner. This information dictates whether the stroke team can safely give a thrombolytic medication (e.g., TNK) or if they must pivot to an alternate therapy. When passing the patient over, you should provide the following for anticoagulant history:
- Drug name (e.g., Apixaban, Rivaroxaban, Warfarin)
- Dose prescribed
- Date and exact time the last dose was taken
Incapacity & Consent:
Acute stroke patients may be unable to provide informed consent due to aphasia, cognitive impairment, or reduced level of consciousness. When possible, identify the Substitute Decision Maker (SDM) or Power of Attorney (POA) while still on scene. Document their name, relationship to the patient, and contact information. This information can help the receiving physician obtain consent for time-sensitive interventions without unnecessary delays.
Time is brain - but accurate information drives treatment decisions. Before leaving the scene, ensure you have documented:
- The source of the Last Seen Normal (LSN) time
- The name, dose, and timing of any anticoagulant or antiplatelet medications
- SDM/POA contact information, when applicable
The quality of the information you provide can be just as important as the speed with which you provide it.
When establishing the timeline for a stroke or altered patient, avoid relying solely on vague statements such as "they woke up like this." Instead, use specific anchor points to verify timing, such as:
- The last phone call, text message, or social interaction
- The last meal or beverage consumed
- A witnessed activity, appointment, or television program
Cross-referencing multiple timeline anchors can improve the accuracy of the LSN and support timely stroke treatment decisions.
Additional stroke resources are available through the Northwestern Ontario Regional Stroke Network.