
July 2026 - Tip of the Month - Early Transport Decisions in Cardiac Arrest
Early Transport Decisions in Cardiac Arrest
Out-of-hospital cardiac arrest management requires paramedics to balance the benefits of on-scene resuscitation with the potential advantages of rapid transport. High-quality CPR, rhythm analysis, defibrillation, and airway management are often best performed in a controlled on-scene environment. However, some patients who are unlikely to meet Termination of Resuscitation (TOR) criteria may benefit from early transport, and this is not limited to the H’s and T’s of reversible causes. The decision to transport prior to 20 minutes of resuscitation should be guided by objective clinical factors and the ability to maintain high-quality resuscitation throughout extrication and transport.
By the end of this tip, paramedics will be able to identify key clinical factors that should guide decisions regarding early transport during cardiac arrest resuscitation.
You are managing a 54-year-old patient in cardiac arrest with persistent, narrow complex PEA. High-quality CPR is ongoing with an automated CPR device, the airway is managed with a supraglottic airway, there are ample resources on scene for a simple extrication and transport time to the nearest emergency department is less than five minutes. Do you remain on scene to continue resuscitation for 20 minutes, or initiate early transport?
Deciding to leave the scene prior to 20 minutes of resuscitation should never be based on intuition, pressure from bystanders, or a desire to “do more.” Decisions should be based on objective clinical findings and what is most beneficial for the patient.
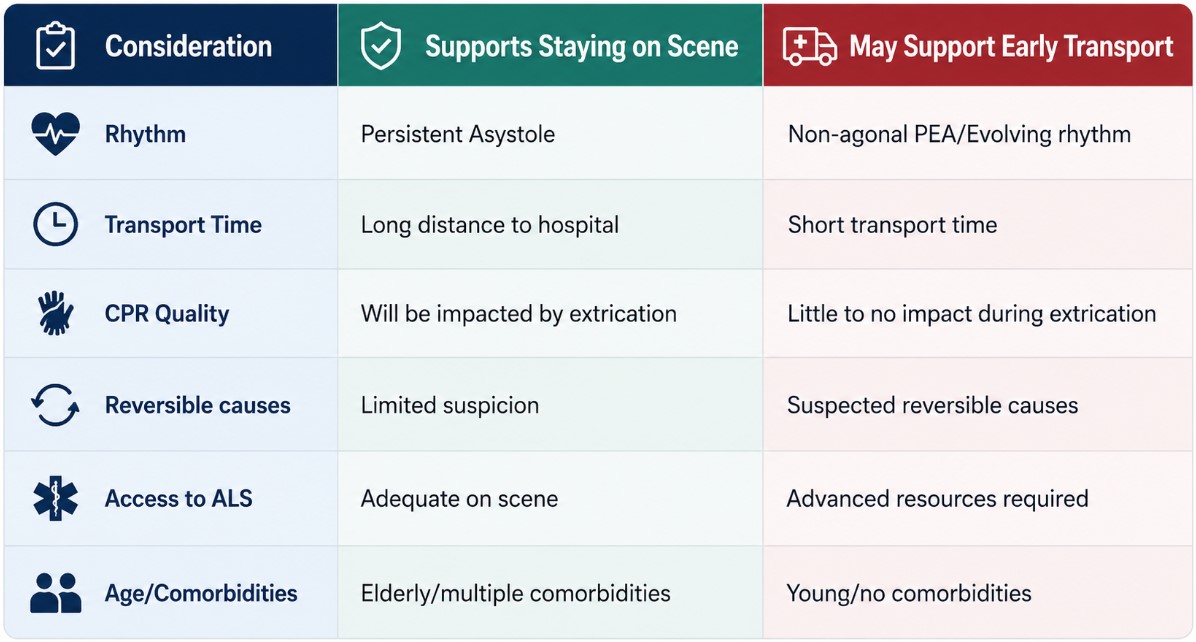
Consider the full clinical picture. Factors that may influence the decision to transport early include: Suspected cause of arrest, patient age, distance to hospital, access to ACLS interventions, presenting and evolving cardiac rhythm, reversible causes, and ability to maintain high quality CPR during movement and transport.
High quality CPR remains the priority. Transporting a patient should not come at the expense of effective resuscitation. If CPR quality, rhythm interpretations, ventilation or medication administration will be significantly compromised during extrication or transport, remaining on scene may provide the patient with the best opportunity for survival.
Paramedics may initiate transport before 20 minutes of on-scene resuscitation when the decision is supported by objective clinical factors and high-quality resuscitation can be maintained during extrication and transport. The decision must not be based solely on intuition, time pressure, or external pressure.
During your next cardiac arrest call, ask yourself: “will transporting this patient improve access to meaningful interventions without compromising resuscitation efforts?”